Shifting left? An analysis of health prevention policies in the 10 Year Health Plan
In brief
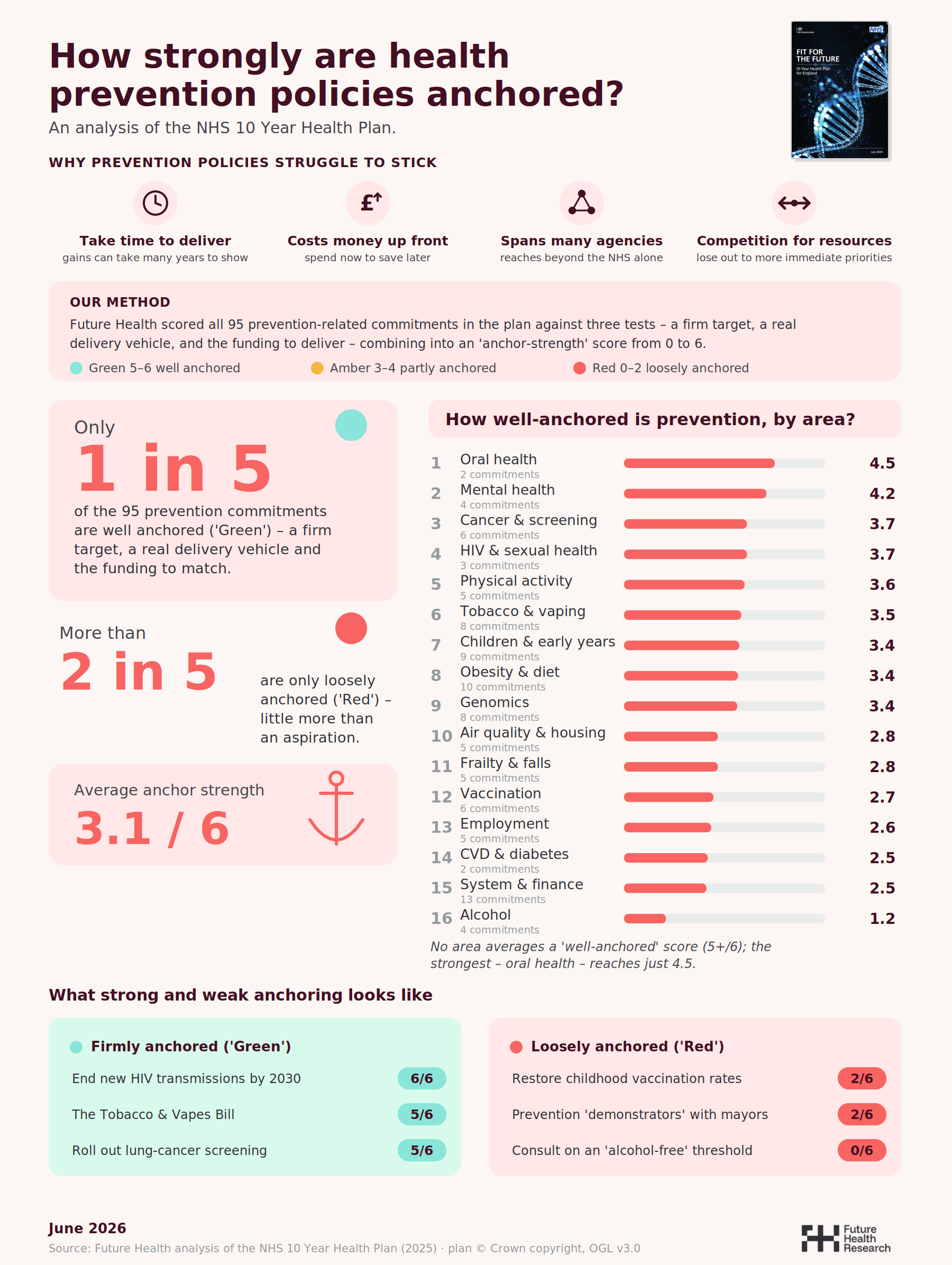
A year on from publication, this short research paper asks a simple question of the NHS 10 Year Health Plan: not how ambitious its prevention agenda is, but how firmly it is anchored. We scored all 95 prevention-related commitments in the plan against three tests – a firm target, a real delivery vehicle, and the funding to deliver – to produce an ‘anchor-strength’ score for each. The picture is of a plan with plenty of prevention ambition but thin on clear deliverable commitments.
Only around one in five commitments is well anchored; more than two in five are little more than an aspiration. No single area of prevention scores, on average, as well anchored. Moving from sickness to prevention is one of the plan’s three shifts, but without firm anchors in place many of the commitments in the plan are unlikely to be realised.
Background: Why prevention is hard to anchor
Every health secretary of the past quarter-century has promised to shift the NHS “from sickness to prevention” (indeed the first major statement of this ambition, the discussion paper Prevention and Health: Everybody’s Business, appeared in 1976). The ambition is not new, and nor is the diagnosis behind it. More than twenty years ago the Treasury-commissioned Wanless reviews warned that, without a “fully engaged” population and sustained investment in prevention, demand on the NHS would outstrip any plausible increase in funding. The case for prevention has been made, repeatedly and authoritatively, for a generation.
And yet prevention has remained the part of health policy most prone to slipping. There are four well-established structural reasons why:
Prevention takes time to deliver. The benefits of stopping people becoming ill accrue over years and often decades, well beyond the electoral and fiscal cycles in which decisions are made. A smoke-free generation, a fall in childhood obesity, a narrowing of the healthy-life-expectancy gap: none of these can be banked inside a single Parliament. The political reward arrives long after the political cost.
Prevention requires money up front. Prevention is an investment that requires upfront investment for apotential return later, which makes it perennially vulnerable when budgets are tight. The clearest illustration is the public health grant – the ring-fenced budget local authorities use to fund stop-smoking services, sexual health, drug and alcohol treatment and children’s health. It has been cut by 28% per person in real terms since 2015/16. This is despite strong value-for-money evidence: the Health Foundation estimates that an additional year of good health bought through public-health interventions costs around £3,800, three to four times cheaper than the equivalent gain from NHS treatment.
Prevention spans many agencies. The biggest drivers of ill health – tobacco, alcohol, diet, housing, air quality, income, work – sit largely outside the NHS, across local government and other Whitehall departments. As the Marmot reviews of health inequalities have long argued, the conditions in which people live and work shape their health more than the health service does. That makes prevention a genuinely cross-government enterprise, and cross-government enterprises are hard to own, hard to fund and hard to hold to account.
Prevention competes for resources. Faced with a choice between an immediate, visible pressure – the waiting list, the A&E winter, the elective backlog – and a long-term, invisible gain, the urgent almost always wins. Prevention loses out to more immediate priorities, not because anyone disputes its value, but because the system that allocates money and attention is built around acute demand.
These four pressures are why ambition in prevention and making a high level case for shifting towards it is in many ways the easy part.
What is harder is whether a prevention commitment is anchored: tied down firmly enough to survive the years, the budget rounds, the departmental hand-offs and the competition for attention that would otherwise let it drift.
This short report looks to assess how strong the Government’s prevention policy commitments are.
Method: assessing how Government prevention policy is anchored
We read the NHS 10 Year Health Plan for England in full and identified every commitment with a preventative purpose, across the prevention spectrum: averting disease before it arises (primary prevention); detecting and intervening early to stop it progressing, such as screening (secondary prevention); and limiting complications and deterioration in those with established conditions (tertiary prevention). We coded by intent, not by setting – a measure counts whether it is delivered in a hospital, a pharmacy, a GP surgery or a school – and we set aside commitments concerned purely with treating or managing acute illness. On that basis we identified 95 prevention-related commitments: 52 primary, 24 secondary and 3 tertiary, together with 16 “enabling” commitments that build the infrastructure prevention depends on, such as data, genomics and population-health tools.
We then scored each commitment from 0 to 2 on three tests, and summed them into an “anchor-strength” score out of 6:
- Target – is there a firm, measurable, time-bound aim? (0 = none; 1 = a direction of travel; 2 = a quantified aim with a deadline)
- Delivery vehicle – is there a real mechanism to make it happen? (0 = aspiration or consultation; 1 = a pilot or programme; 2 = legislation, a contract, or a funded national programme)
- Funding – is money attached and evidenced? (0 = none; 1 = partial or indirect; 2 = funded and costed)
We banded the results using a simple traffic-light scale: Green (5–6) well anchored; Amber (3–4) partly anchored; Red (0–2) loosely anchored.
Five points of scope are worth stating plainly. First, this is an assessment of how firmly commitments are pinned down, not of whether they are good policy or likely to work – a well-designed idea can be weakly anchored, and a firmly anchored one can be misguided. Second, this analysis is a snapshot of policy anchoring – looking at three elements – targets, delivery vehicles, funding – there are a plethora of other ways in which policies can be anchored (other examples include Ministerial champions, alignment to wider Government agendas – e.g. growth, and the evidence base for change) but these are arguably three of the most significant. Third, we only reviewed the Ten Year Health Plan, as the most recent national policy document covering the Government’s proposed shift to prevention. Further analysis is planned to look at progress on these commitments in the months ahead. Fourth, we deliberately did not score the plan’s overarching mission to halve the gap in healthy life expectancy. It sits above the 95 commitments as a defining aspiration rather than as a discrete, measurable commitment. Fifth, for the area ranking each commitment is assigned to a single primary area to avoid double-counting; some commitments are genuinely cross-cutting – HPV vaccination, for example, is both an immunisation and a cancer-prevention measure – so the area averages are indicative, and a thematic reading may legitimately draw on commitments filed under more than one area.
Analysis: what we found
The headline picture
Across the 95 commitments, only 18 (19%) are well anchored (Green). 37 (39%) are partly anchored (Amber), and 40 (42%) are loosely anchored (Red). The mean anchor-strength score is 3.1 out of 6.
Put plainly: only around one in five of the plan’s prevention promises carries a firm target, a real delivery vehicle and the funding to match. More than two in five are little more than an aspiration – a stated intention without the apparatus to deliver it.
No area of prevention is, on average, well anchored
Grouping the commitments into sixteen areas of prevention reveals a consistent picture: not one area averages a well-anchored (Green) score. The strongest – oral health – reaches 4.5 out of 6, and even that rests on only two commitments. Mental health follows at 4.2; cancer and screening, and HIV and sexual health, sit at 3.7. At the other end, alcohol scores 1.25, the weakest of any area by some distance, followed by the cluster of system and finance “enablers” (2.5), CVD and diabetes (2.5), employment (2.6), vaccination (2.7), and frailty and falls (2.8).
No single area of prevention scores, on average, as well anchored. The strongest – oral health – reaches 4.5 out of 6.
What good anchoring looks like
The well-anchored commitments share a common feature: something external holds them in place. They tend to rest on one of three firm foundations.
- A statute. The Tobacco and Vapes Bill is the clearest example: a legislative spine that survives changes of minister and budget.
- A dated, quantified target. The pledge to end new HIV transmissions in England by 2030 scores a full 6: a specific outcome, a deadline, an action plan and funding behind it.
- A funded national programme. The roll-out of lung-cancer screening to those with a smoking history scores 5 – a concrete, resourced programme with national reach.
These are the templates. Where prevention is anchored, it is anchored because it has been pinned to a law, a date, or a funded delivery machine.
“Anchored headline, weak delivery tail”
A striking and recurrent pattern is that a firm headline commitment often sits above a set of unanchored delivery mechanisms. The destination is fixed; the route is not.
Tobacco is the sharpest case: a world-leading statutory commitment to a smoke-free generation (Green), above stop-smoking tools that are loosely anchored (Red). HIV shows the same shape: a clean 2030 elimination target (Green), but the equity ambitions riding on it – improving PrEP access and reaching under-served communities – are themselves only loosely anchored. The plan commits to where it wants to get to far more firmly than to how it will get there.
This is not necessarily a problem if subsequent policy documentation can flesh out these details, but the danger is that the lack of a delivery chapter of the Ten Year Health Plan creates a gap between pledge and commitment, which itself can create difficulties in effective policy execution.
Borrowed anchors: often someone else’s money
A large share of the most firmly anchored prevention commitments are not, on closer inspection, NHS commitments at all. They score well precisely because another department has already committed the budget:
- Free school meals for all children with a parent on Universal Credit (Department for Education);
- Investment in grassroots sport and physical activity (DCMS and Sport England);
- £616m for active travel (Department for Transport);
- The £13.2bn Warm Homes plan (Department for Energy Security and Net Zero).
These are genuine, well-anchored prevention measures, and the plan is right to claim them. But strip out the commitments funded and owned beyond the NHS, and the stock of firmly anchored prevention that the health system itself owns and pays for is thinner than the plan’s framing implies. This is not a criticism of cross-government working – prevention should be cross-government – but it does mean the plan’s prevention strength is, in part, borrowed.
The weakest links: alcohol, vaccination, and the delivery machinery
The analysis reveals three areas of weakness.
Alcohol is the least-anchored area in the entire plan (1.25/6). Its flagship measures – a consultation on an “alcohol-free” labelling threshold, exploring restrictions on no- and low-alcohol products – are consultations and explorations, not commitments. For a leading preventable cause of harm, this is conspicuous.
Vaccination scores poorly (2.7/6) at exactly the moment childhood immunisation rates are falling. The intention to restore uptake is clear, but the commitments behind it – improving school consent processes, working with local government to rebuild confidence – are loosely anchored aspirations rather than funded, time-bound programmes. A critical public-health objective rests on soft commitments.
The delivery machinery is itself unfunded. This is perhaps the most consequential finding. The plan rests much of its prevention case on the system “enablers” – the Neighbourhood Health Service, prevention “demonstrators” with mayors, community health and wellbeing workers, the financial incentives meant to make prevention pay. As a group these score just 2.5/6, and not one of them is well anchored.
The mission with no anchor
Finally, the plan’s defining prevention ambition – to halve the gap in healthy life expectancy between the richest and poorest areas – sits above all of this as a broad aspiration. There is little detail on how this will be achieved and how the plan’s constituent parts add up to deliver it.
Conclusion and implications
The challenges with prevention related health policy are well documented. The Ten Year Health Plan unfortunately demonstrates many of the weaknesses that have been seen in national policy on prevention before: particularly a focus on high level narratives and commitments without strong anchors – specifically targets, delivery vehicles and funding.
This means that whilst there may be some progress on particular issues and policies that are more strongly anchored in the plan (e.g. tobacco control), the majority lack the anchors that delivery usually requires. This will ultimately mean that the left-shift to prevention will remain an ambition rather than a reality.
When making a case for prevention related health policies, there is an urgent need to move beyond ambition and rhetoric and instead what is needed is a clearer-eyed focus on what is required to deliver and anchor preventative health policy effectively:
- What is the problem? (i.e. what is the specific issue we need to address)
- Why is this problem important? (i.e. scale of the problem, relation to larger problems etc.)
- What is required to address it? (i.e. what is the evidence for change – intervention + outcome)
- Who/what is the delivery vehicle for change? (i.e. who is both accountable and who is responsible for delivery)
- What investment is needed? (i.e. what scale, where will it come from, and what will need to be stopped/diverted to support it)
- What target / goals should we set? (i.e. what is achievable, how can we track progress)
At the macro Government level there should be a small set of indicators that the Government uses to track its prevention related health policy goals and progress on the left shift.
Prevention in health policy is not impossible: smoking, Sure Start and teenage pregnancy rates are just three examples of where progress has been made. But to succeed the right policy architecture is needed.
This analysis shows that the wait for that unfortunately goes on.
If you would like the full data tables behind the analysis please contact Richard at richard@futurehealth-research.com